What Causes Heel Pain And Discomfort
Overview

Heel pain can be very aggravating, especially when taking those first steps in the morning. The key to decreasing and possibly eliminating heel pain is to stretch your heel cord and plantar fascia. The heel cord is the Achilles tendon, which connects the gastrocnemius and soleus muscles in the calf to the heel bone. The plantar fascia is a thick tissue that runs along the bottom of your foot, connecting the heel bone to the toes and maintaining the arch.
Causes
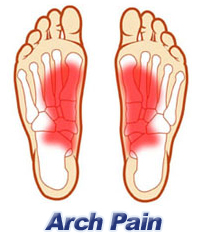
There are many causes of heel pain. However, plantar fasciitis, also known as heel spur syndrome, is the most common, by far. The pain is usually localized to the bottom of the heel towards the inside of the foot. The arch may also be painful. With this condition, pain is typically most severe with the first few steps after a period of rest. The pain my then subside and then return after extended periods of standing. There is usually no specific traumatic event that is responsible for the condition. It is usually the result of overuse, e.g. too much standing, walking or running. There are several common contributory factors such as weight gain, foot type, shoes. Flat shoes or going barefoot are the worst. Athletic shoes are usually the best. The plantar fascia is a fibrous band or ligament that connects the ball of the foot with the heel and helps to support the arch. When this band gets stretched too much or overused, inflammation results, often at the location where it attaches to the heel bone. A heel spur may develop as a result of chronic pulling by the plantar fascia. However, it should be noted that the pain is not caused by the spur. In fact, in some of the most severe cases, there is no spur at all. In other instances, an X-ray may be taken for an unrelated condition and an extremely large but non-painful spur may be seen. Other causes of heel pain include gout, stress fracture, bone tumors, nerve entrapment and thinning of the fat pad beneath the heel. Pain at the back of the heel is usually not plantar fasciitis. (Pain at the back of the heel is often due to an inflammation of the Achilles tendon, enlargement of the heel bone or bursitis.)
Symptoms
Symptoms include a dull ache which is felt most of the time with episodes of a sharp pain in the centre of the heel or on the inside margin of the heel. Often the pain is worse on first rising in the morning and after rest and is aggravated by prolonged weight bearing & thin soled shoes.
Diagnosis
A podiatrist (doctor who specializes in the evaluation and treatment of foot diseases) will carry out a physical examination, and ask pertinent questions about the pain. The doctor will also ask the patient how much walking and standing the patient does, what type of footwear is worn, and details of the his/her medical history. Often this is enough to make a diagnosis. Sometimes further diagnostic tests are needed, such as blood tests and imaging scans.
Non Surgical Treatment
Morning Wall Stretch. Stand barefoot in front of wall, as shown. Press into wall with both hands and lean forward, feeling stretch along back of left leg and heel. Hold for 30 seconds; switch sides and repeat. Freeze and Roll. Freeze a small water bottle. Cover it with a towel and place arch of your foot on top of it. Slowly roll bottle beneath arch of foot for about 5 minutes at a time. Switch sides and repeat. Rub It Out. Use both thumbs to apply deep pressure along arch of the feet, heel, and calf muscles, moving slowly and evenly. Continue for 1 minute. Switch sides and repeat. If you foot pain isn't improving or worsens after 2 weeks, a podiatrist or othopedist can prescribe additional therapies to alleviate discomfort and prevent recurrence.
Surgical Treatment
Although most patients with plantar fasciitis respond to non-surgical treatment, a small percentage of patients may require surgery. If, after several months of non-surgical treatment, you continue to have heel pain, surgery will be considered. Your foot and ankle surgeon will discuss the surgical options with you and determine which approach would be most beneficial for you. No matter what kind of treatment you undergo for plantar fasciitis, the underlying causes that led to this condition may remain. Therefore, you will need to continue with preventive measures. Wearing supportive shoes, stretching, and using custom orthotic devices are the mainstay of long-term treatment for plantar fasciitis.
heel pad anatomy
Prevention
You can reduce the risk of heel pain in many ways, including. Wear shoes that fit you properly with a firm fastening, such as laces. Choose shoes with shock-absorbent soles and supportive heels. Repair or throw out any shoes that have worn heels. Always warm up and cool down when exercising or playing sport, include plenty of slow, sustained stretches. If necessary, your podiatrist will show you how to tape or strap your feet to help support the muscles and ligaments. Shoe inserts (orthoses) professionally fitted by your podiatrist can help support your feet in the long term.
Heel pain can be very aggravating, especially when taking those first steps in the morning. The key to decreasing and possibly eliminating heel pain is to stretch your heel cord and plantar fascia. The heel cord is the Achilles tendon, which connects the gastrocnemius and soleus muscles in the calf to the heel bone. The plantar fascia is a thick tissue that runs along the bottom of your foot, connecting the heel bone to the toes and maintaining the arch.
Causes
There are many causes of heel pain. However, plantar fasciitis, also known as heel spur syndrome, is the most common, by far. The pain is usually localized to the bottom of the heel towards the inside of the foot. The arch may also be painful. With this condition, pain is typically most severe with the first few steps after a period of rest. The pain my then subside and then return after extended periods of standing. There is usually no specific traumatic event that is responsible for the condition. It is usually the result of overuse, e.g. too much standing, walking or running. There are several common contributory factors such as weight gain, foot type, shoes. Flat shoes or going barefoot are the worst. Athletic shoes are usually the best. The plantar fascia is a fibrous band or ligament that connects the ball of the foot with the heel and helps to support the arch. When this band gets stretched too much or overused, inflammation results, often at the location where it attaches to the heel bone. A heel spur may develop as a result of chronic pulling by the plantar fascia. However, it should be noted that the pain is not caused by the spur. In fact, in some of the most severe cases, there is no spur at all. In other instances, an X-ray may be taken for an unrelated condition and an extremely large but non-painful spur may be seen. Other causes of heel pain include gout, stress fracture, bone tumors, nerve entrapment and thinning of the fat pad beneath the heel. Pain at the back of the heel is usually not plantar fasciitis. (Pain at the back of the heel is often due to an inflammation of the Achilles tendon, enlargement of the heel bone or bursitis.)
Symptoms
Symptoms include a dull ache which is felt most of the time with episodes of a sharp pain in the centre of the heel or on the inside margin of the heel. Often the pain is worse on first rising in the morning and after rest and is aggravated by prolonged weight bearing & thin soled shoes.
Diagnosis
A podiatrist (doctor who specializes in the evaluation and treatment of foot diseases) will carry out a physical examination, and ask pertinent questions about the pain. The doctor will also ask the patient how much walking and standing the patient does, what type of footwear is worn, and details of the his/her medical history. Often this is enough to make a diagnosis. Sometimes further diagnostic tests are needed, such as blood tests and imaging scans.
Non Surgical Treatment
Morning Wall Stretch. Stand barefoot in front of wall, as shown. Press into wall with both hands and lean forward, feeling stretch along back of left leg and heel. Hold for 30 seconds; switch sides and repeat. Freeze and Roll. Freeze a small water bottle. Cover it with a towel and place arch of your foot on top of it. Slowly roll bottle beneath arch of foot for about 5 minutes at a time. Switch sides and repeat. Rub It Out. Use both thumbs to apply deep pressure along arch of the feet, heel, and calf muscles, moving slowly and evenly. Continue for 1 minute. Switch sides and repeat. If you foot pain isn't improving or worsens after 2 weeks, a podiatrist or othopedist can prescribe additional therapies to alleviate discomfort and prevent recurrence.
Surgical Treatment
Although most patients with plantar fasciitis respond to non-surgical treatment, a small percentage of patients may require surgery. If, after several months of non-surgical treatment, you continue to have heel pain, surgery will be considered. Your foot and ankle surgeon will discuss the surgical options with you and determine which approach would be most beneficial for you. No matter what kind of treatment you undergo for plantar fasciitis, the underlying causes that led to this condition may remain. Therefore, you will need to continue with preventive measures. Wearing supportive shoes, stretching, and using custom orthotic devices are the mainstay of long-term treatment for plantar fasciitis.
heel pad anatomy
Prevention
You can reduce the risk of heel pain in many ways, including. Wear shoes that fit you properly with a firm fastening, such as laces. Choose shoes with shock-absorbent soles and supportive heels. Repair or throw out any shoes that have worn heels. Always warm up and cool down when exercising or playing sport, include plenty of slow, sustained stretches. If necessary, your podiatrist will show you how to tape or strap your feet to help support the muscles and ligaments. Shoe inserts (orthoses) professionally fitted by your podiatrist can help support your feet in the long term.
How To Handle Fallen Arches
Overview
Most people (approx. 60-70% of the population) suffer from excessive pronation due to flat feet when walking, running and standing. Though the foot may appear normal when sitting down, with a clear arch present under the foot, over-pronation becomes noticeable when we stand or walk as a result of weight bearing. The arches collapse with every step we take, and the ankles roll inwards. This is called overpronation, a biomechanical imbalance that can lead to many painful foot conditions such as heel pain, plantar fasciitis, heel spurs, tendonitis, and can even affect other parts of your body such as the knees and lower back.
Causes
There are several factors that can contribute to the development of fallen arches. These factors include the following. Genetic abnormality, torn or stretched tendons, amage to the posterior tibial tendon, bone fractures, dislocation of bones, nerve damage, rheumatoid arthritis and other medical conditions. In addition, there are other factors that can increase your risk of developing fallen arches. These risk factors include diabetes, pregnancy, Obesity and Aging.
Symptoms
The primary symptom of fallen arches is painful or achy feet in the area in which the foot arches or on the heel. This area may become swollen and painful to stand still on. This causes the patient to improperly balance on their feet which in turn will cause other biomechanical injuries such as back, leg and knee pain.
Diagnosis
If you notice that your feet are flat, but you?re not really experiencing any pain, then you?re probably okay to go without a visit to the podiatrist (unless, of course, you have a lack of feeling in your foot). You can schedule a hair appointment instead, or maybe see a movie. However, once painful symptoms start to appear, it?s better to skip the hirsute (or cinematic) experience and go see your foot doctor. Your podiatrist will likely make the diagnosis by examining your foot visually, asking about symptoms you may be experiencing, and may test your muscle strength. You may be asked to stand on your toes (in a ballerina pose, if you prefer, although that?s certainly not required), or walk around the examining room, and you may need to show the podiatrist your shoes. He or she may comment on your excellent taste in footwear, but is more likely to check your shoes for signs of wear that may indicate fallen arches. Your podiatrist may recommend X-rays, a CT scan or an MRI in order to get a look at the interior of your foot, although the best diagnosis usually comes from the doctor?s own in-person examination.
best arch support insoles for plantar fasciitis
Non Surgical Treatment
There are home remedies to prevent or manage pain from fallen arches or flat feet. Here are some areas to consider. Wear footwear or shoe inserts that are appropriate to your activity. When pain occurs, try at-home treatment of rest, ice, and over-the-counter nonsteroidal anti-inflammatories, or NSAIDS, such as ibuprofen. Ask your doctor or a physical therapist to show you stretches that can prepare you for feet-intensive activities. Limit or treat risk factors that can make fallen arches or flat feet worse, such as diabetes, high blood pressure, and obesity. Avoid activities that put excessive stress on your feet, such as running on roads. Avoid high-impact sports such as basketball, hockey, soccer, and tennis. Know when to get help. When pain is severe or interferes with activities, it's time to see the doctor for a thorough exam and treatment.
Surgical Treatment

Generally one of the following procedures is used to surgically repair a flat foot or fallen arch. Arthrodesis. One or more of your bones in the foot or ankle are fused together. Osteotomy. Correcting alignment by cutting and reshaping a bone. Excision. Removing a bone or a bone spur. Synovectomy. Cleaning the sheath that covers the tendon. Tendon transfer. Using a piece of one tendon to lengthen or replace another. Arthroereisis. placing a small device in the subtalar joint to limit motion. For most people, treatment is successful, regardless of the cause, although the cause does does play a major role in determining your prognosis. Some causes do not need treatment, while others require a surgical fix.
Most people (approx. 60-70% of the population) suffer from excessive pronation due to flat feet when walking, running and standing. Though the foot may appear normal when sitting down, with a clear arch present under the foot, over-pronation becomes noticeable when we stand or walk as a result of weight bearing. The arches collapse with every step we take, and the ankles roll inwards. This is called overpronation, a biomechanical imbalance that can lead to many painful foot conditions such as heel pain, plantar fasciitis, heel spurs, tendonitis, and can even affect other parts of your body such as the knees and lower back.
Causes
There are several factors that can contribute to the development of fallen arches. These factors include the following. Genetic abnormality, torn or stretched tendons, amage to the posterior tibial tendon, bone fractures, dislocation of bones, nerve damage, rheumatoid arthritis and other medical conditions. In addition, there are other factors that can increase your risk of developing fallen arches. These risk factors include diabetes, pregnancy, Obesity and Aging.
Symptoms
The primary symptom of fallen arches is painful or achy feet in the area in which the foot arches or on the heel. This area may become swollen and painful to stand still on. This causes the patient to improperly balance on their feet which in turn will cause other biomechanical injuries such as back, leg and knee pain.
Diagnosis
If you notice that your feet are flat, but you?re not really experiencing any pain, then you?re probably okay to go without a visit to the podiatrist (unless, of course, you have a lack of feeling in your foot). You can schedule a hair appointment instead, or maybe see a movie. However, once painful symptoms start to appear, it?s better to skip the hirsute (or cinematic) experience and go see your foot doctor. Your podiatrist will likely make the diagnosis by examining your foot visually, asking about symptoms you may be experiencing, and may test your muscle strength. You may be asked to stand on your toes (in a ballerina pose, if you prefer, although that?s certainly not required), or walk around the examining room, and you may need to show the podiatrist your shoes. He or she may comment on your excellent taste in footwear, but is more likely to check your shoes for signs of wear that may indicate fallen arches. Your podiatrist may recommend X-rays, a CT scan or an MRI in order to get a look at the interior of your foot, although the best diagnosis usually comes from the doctor?s own in-person examination.
best arch support insoles for plantar fasciitis
Non Surgical Treatment
There are home remedies to prevent or manage pain from fallen arches or flat feet. Here are some areas to consider. Wear footwear or shoe inserts that are appropriate to your activity. When pain occurs, try at-home treatment of rest, ice, and over-the-counter nonsteroidal anti-inflammatories, or NSAIDS, such as ibuprofen. Ask your doctor or a physical therapist to show you stretches that can prepare you for feet-intensive activities. Limit or treat risk factors that can make fallen arches or flat feet worse, such as diabetes, high blood pressure, and obesity. Avoid activities that put excessive stress on your feet, such as running on roads. Avoid high-impact sports such as basketball, hockey, soccer, and tennis. Know when to get help. When pain is severe or interferes with activities, it's time to see the doctor for a thorough exam and treatment.
Surgical Treatment
Generally one of the following procedures is used to surgically repair a flat foot or fallen arch. Arthrodesis. One or more of your bones in the foot or ankle are fused together. Osteotomy. Correcting alignment by cutting and reshaping a bone. Excision. Removing a bone or a bone spur. Synovectomy. Cleaning the sheath that covers the tendon. Tendon transfer. Using a piece of one tendon to lengthen or replace another. Arthroereisis. placing a small device in the subtalar joint to limit motion. For most people, treatment is successful, regardless of the cause, although the cause does does play a major role in determining your prognosis. Some causes do not need treatment, while others require a surgical fix.
Leg Length Discrepancy Gait Cycle
Overview
Surgical lengthening of the shorter extremity (upper or lower) is another treatment option. The bone is lengthened by surgically applying an external fixator to the extremity in the operating room. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins or both. A small crack is made in the bone and tension is created by the frame when it is "distracted" by the patient or family member who turns an affixed dial several times daily. The lengthening process begins approximately five to ten days after surgery. The bone may lengthen one millimeter per day, or approximately one inch per month. Lengthening may be slower in adults overall and in a bone that has been previously injured or undergone prior surgery. Bones in patients with potential blood vessel abnormalities (i.e., cigarette smokers) may also lengthen more slowly. The external fixator is worn until the bone is strong enough to support the patient safely, approximately three months per inch of lengthening. This may vary, however, due to factors such as age, health, smoking, participation in rehabilitation, etc. Risks of this procedure include infection at the site of wires and pins, stiffness of the adjacent joints and slight over or under correction of the bone?s length. Lengthening requires regular follow up visits to the physician?s office, meticulous hygiene of the pins and wires, diligent adjustment of the frame several times daily and rehabilitation as prescribed by your physician.
Causes
A number of causes may lead to leg length discrepancy in children. Differences in leg length frequently follow fractures in the lower extremities in children due to over or under stimulation of the growth plates in the broken leg. Leg length discrepancy may also be caused by a congenital abnormality associated with a condition called hemihypertrophy. Or it may result from neuromuscular diseases such as polio and cerebral palsy. Many times, no cause can be identified. A small leg length discrepancy of a quarter of an inch or less is quite common in the general population and of no clinical significance. Larger leg length discrepancies become more significant. The long-term consequences of a short leg may include knee pain, back pain, and abnormal gait or limp.
Symptoms
The effects of a short leg depend upon the individual and the extent of discrepancy. The most common manifestation if a lateral deviation of the lumbar spine toward the short side with compensatory curves up the spine that can extend into the neck and even impacts the TMJ. Studies have shown that anterior and posterior curve abnormalities also can result.
Diagnosis
On standing examination one iliac crest may be higher/lower than the other. However a physiotherapist, osteopath or chiropractor will examine the LLD in prone or supine position and measure it, confirming the diagnosis of structural (or functional) LLD. The LLD should be measured using bony fixed points. X-Ray should be taken in a standing position. The osteopath, physiotherapist or chiropractor will look at femoral head & acetabulum, knee joints, ankle joints.
Non Surgical Treatment
In some circumstances, the physician will recommend a non-surgical form of treatment. Non-surgical treatments include orthotics and prosthetics. Orthotics are a special type of lift placed in or on a shoe that can be used in the treatment of leg length discrepancies between two and six centimeters. In pediatric patients who have large discrepancies and are not good candidates for other treatment forms, prosthetics can be helpful.

how to increase height in 1 week
Surgical Treatment
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
Surgical lengthening of the shorter extremity (upper or lower) is another treatment option. The bone is lengthened by surgically applying an external fixator to the extremity in the operating room. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins or both. A small crack is made in the bone and tension is created by the frame when it is "distracted" by the patient or family member who turns an affixed dial several times daily. The lengthening process begins approximately five to ten days after surgery. The bone may lengthen one millimeter per day, or approximately one inch per month. Lengthening may be slower in adults overall and in a bone that has been previously injured or undergone prior surgery. Bones in patients with potential blood vessel abnormalities (i.e., cigarette smokers) may also lengthen more slowly. The external fixator is worn until the bone is strong enough to support the patient safely, approximately three months per inch of lengthening. This may vary, however, due to factors such as age, health, smoking, participation in rehabilitation, etc. Risks of this procedure include infection at the site of wires and pins, stiffness of the adjacent joints and slight over or under correction of the bone?s length. Lengthening requires regular follow up visits to the physician?s office, meticulous hygiene of the pins and wires, diligent adjustment of the frame several times daily and rehabilitation as prescribed by your physician.
Causes
A number of causes may lead to leg length discrepancy in children. Differences in leg length frequently follow fractures in the lower extremities in children due to over or under stimulation of the growth plates in the broken leg. Leg length discrepancy may also be caused by a congenital abnormality associated with a condition called hemihypertrophy. Or it may result from neuromuscular diseases such as polio and cerebral palsy. Many times, no cause can be identified. A small leg length discrepancy of a quarter of an inch or less is quite common in the general population and of no clinical significance. Larger leg length discrepancies become more significant. The long-term consequences of a short leg may include knee pain, back pain, and abnormal gait or limp.
Symptoms
The effects of a short leg depend upon the individual and the extent of discrepancy. The most common manifestation if a lateral deviation of the lumbar spine toward the short side with compensatory curves up the spine that can extend into the neck and even impacts the TMJ. Studies have shown that anterior and posterior curve abnormalities also can result.
Diagnosis
On standing examination one iliac crest may be higher/lower than the other. However a physiotherapist, osteopath or chiropractor will examine the LLD in prone or supine position and measure it, confirming the diagnosis of structural (or functional) LLD. The LLD should be measured using bony fixed points. X-Ray should be taken in a standing position. The osteopath, physiotherapist or chiropractor will look at femoral head & acetabulum, knee joints, ankle joints.
Non Surgical Treatment
In some circumstances, the physician will recommend a non-surgical form of treatment. Non-surgical treatments include orthotics and prosthetics. Orthotics are a special type of lift placed in or on a shoe that can be used in the treatment of leg length discrepancies between two and six centimeters. In pediatric patients who have large discrepancies and are not good candidates for other treatment forms, prosthetics can be helpful.
how to increase height in 1 week
Surgical Treatment
Lengthening is usually done by corticotomy and gradual distraction. This technique can result in lengthenings of 25% or more, but typically lengthening of 15%, or about 6 cm, is recommended. The limits of lengthening depend on patient tolerance, bony consolidation, maintenance of range of motion, and stability of the joints above and below the lengthened limb. Numerous fixation devices are available, such as the ring fixator with fine wires, monolateral fixator with half pins, or a hybrid frame. The choice of fixation device depends on the desired goal. A monolateral device is easier to apply and better tolerated by the patient. The disadvantages of monolateral fixation devices include the limitation of the degree of angular correction that can concurrently be obtained; the cantilever effect on the pins, which may result in angular deformity, especially when lengthening the femur in large patients; and the difficulty in making adjustments without placing new pins. Monolateral fixators appear to have a similar success rate as circular fixators, especially with more modest lengthenings (20%).
What Is Mortons Neuroma
Overview
 Also known as Morton's Interdigital Neuroma, Morton's Metatarsalgia, Morton's Neuralgia, Plantar Neuroma, Intermetatarsal Neuroma) What is a Morton's neuroma? Morton's neuroma is a condition characterized by localized swelling of the nerve and soft tissue located between two of the long bones of the foot (metatarsals - figure 1), which can result in pain, pins and needles, or numbness in the forefoot or toes.
Also known as Morton's Interdigital Neuroma, Morton's Metatarsalgia, Morton's Neuralgia, Plantar Neuroma, Intermetatarsal Neuroma) What is a Morton's neuroma? Morton's neuroma is a condition characterized by localized swelling of the nerve and soft tissue located between two of the long bones of the foot (metatarsals - figure 1), which can result in pain, pins and needles, or numbness in the forefoot or toes.
Causes
When a nerve is pinched between bones, the result is swelling of the nerve. It is this swelling which is referred to as a Neuroma. When the condition occurs in the foot, it is known as a Morton?s Neuroma. Morton?s Neuroma is technically not a tumor. Rather, it is a thickening of the tissue that surrounds the digital nerves leading to the toes. These nerves allow for physical sensation on the skin of the toes. The region of inflammation is found where the digital nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton?s Neuroma commonly develops between the third and fourth toes, generally as a result of ongoing irritation, trauma or excessive pressure. In some cases, the second and third toes are involved. Morton?s Neuroma is confined to one foot in most cases, though it can occur in both, particularly in athletes such as runners.
Symptoms
Symptoms typically include pain, often with pins and needles on one side of a toe and the adjacent side of the next toe. Pain is made worse by forefoot weight bearing and can also be reproduced by squeezing the forefoot to further compress the nerve. Pressing in between the third and forth metatarsals for example with a pen can also trigger symptoms.
Diagnosis
Your health care provider can usually diagnose this problem by examining your foot. A foot x-ray may be done to rule out bone problems. MRI or high-resolution ultrasound can successfully diagnose Morton's neuroma. Nerve testing (electromyography) cannot diagnose Morton's neuroma, but may be used to rule out conditions that cause similar symptoms. Blood tests may be done to check for inflammation-related conditions, including certain forms of arthritis.
Non Surgical Treatment
Treatment for Morton?s Neuroma usually begins conservatively, with a change in lifestyle choices. People suffering from the condition may find pain relief by reducing activity levels, changing footwear, using orthopedic supports, reducing weight. Medications are also available to help relieve the pain of Morton?s Neuroma. Over-the-counter medications are sometimes very helpful in reducing pain and inflammation. Your health care provider can also provide you with anesthetic or corticosteroid injections. These help to numb the area affected by the neuroma, and reduce inflammation.
Surgical Treatment
Surgery for neuroma most often involves removing affected nerve in the ball of the foot. An incision is made on the top of the foot and the nerve is carefully removed. Surgeon must remove the nerve far enough back so that the nerve doesn?t continue to become impinged at the ball of the foot. Alternatitvely, another type of surgery involves releasing a tight ligament that encases the nerve. Recovery after Morton?s neuroma (neurectomy) surgery is generally quick. Typically patients are walking on the operated foot in a post-surgical shoe for 2 - 4 weeks, depending on healing. Return to shoes is 2-6 weeks after the surgery. Factors that may prolong healing are age, smoking, poor nutritional status, and some medical problems.
Prevention
To help reduce your chance of developing Morton's neuroma avoid wearing tight and/or high-heeled shoes. Maintain or achieve ideal body weight. If you play sports, wear roomy, properly fitting athletic footwear.
Also known as Morton's Interdigital Neuroma, Morton's Metatarsalgia, Morton's Neuralgia, Plantar Neuroma, Intermetatarsal Neuroma) What is a Morton's neuroma? Morton's neuroma is a condition characterized by localized swelling of the nerve and soft tissue located between two of the long bones of the foot (metatarsals - figure 1), which can result in pain, pins and needles, or numbness in the forefoot or toes.Causes
When a nerve is pinched between bones, the result is swelling of the nerve. It is this swelling which is referred to as a Neuroma. When the condition occurs in the foot, it is known as a Morton?s Neuroma. Morton?s Neuroma is technically not a tumor. Rather, it is a thickening of the tissue that surrounds the digital nerves leading to the toes. These nerves allow for physical sensation on the skin of the toes. The region of inflammation is found where the digital nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton?s Neuroma commonly develops between the third and fourth toes, generally as a result of ongoing irritation, trauma or excessive pressure. In some cases, the second and third toes are involved. Morton?s Neuroma is confined to one foot in most cases, though it can occur in both, particularly in athletes such as runners.
Symptoms
Symptoms typically include pain, often with pins and needles on one side of a toe and the adjacent side of the next toe. Pain is made worse by forefoot weight bearing and can also be reproduced by squeezing the forefoot to further compress the nerve. Pressing in between the third and forth metatarsals for example with a pen can also trigger symptoms.
Diagnosis
Your health care provider can usually diagnose this problem by examining your foot. A foot x-ray may be done to rule out bone problems. MRI or high-resolution ultrasound can successfully diagnose Morton's neuroma. Nerve testing (electromyography) cannot diagnose Morton's neuroma, but may be used to rule out conditions that cause similar symptoms. Blood tests may be done to check for inflammation-related conditions, including certain forms of arthritis.
Non Surgical Treatment
Treatment for Morton?s Neuroma usually begins conservatively, with a change in lifestyle choices. People suffering from the condition may find pain relief by reducing activity levels, changing footwear, using orthopedic supports, reducing weight. Medications are also available to help relieve the pain of Morton?s Neuroma. Over-the-counter medications are sometimes very helpful in reducing pain and inflammation. Your health care provider can also provide you with anesthetic or corticosteroid injections. These help to numb the area affected by the neuroma, and reduce inflammation.
Surgical Treatment
Surgery for neuroma most often involves removing affected nerve in the ball of the foot. An incision is made on the top of the foot and the nerve is carefully removed. Surgeon must remove the nerve far enough back so that the nerve doesn?t continue to become impinged at the ball of the foot. Alternatitvely, another type of surgery involves releasing a tight ligament that encases the nerve. Recovery after Morton?s neuroma (neurectomy) surgery is generally quick. Typically patients are walking on the operated foot in a post-surgical shoe for 2 - 4 weeks, depending on healing. Return to shoes is 2-6 weeks after the surgery. Factors that may prolong healing are age, smoking, poor nutritional status, and some medical problems.
Prevention
To help reduce your chance of developing Morton's neuroma avoid wearing tight and/or high-heeled shoes. Maintain or achieve ideal body weight. If you play sports, wear roomy, properly fitting athletic footwear.
Shoe Lifts The Chiropodists Choice For Leg Length Difference
There are actually not one but two different types of leg length discrepancies, congenital and acquired. Congenital implies that you are born with it. One leg is structurally shorter in comparison to the other. Through developmental stages of aging, the brain senses the stride pattern and recognizes some variance. Our bodies usually adapts by tilting one shoulder to the "short" side. A difference of less than a quarter inch is not grossly uncommon, doesn't need Shoe Lifts to compensate and generally doesn't have a serious effect over a lifetime.

Leg length inequality goes largely undiscovered on a daily basis, however this condition is simply corrected, and can reduce quite a few cases of low back pain.
Treatment for leg length inequality commonly consists of Shoe Lifts . Many are affordable, generally costing under twenty dollars, in comparison to a custom orthotic of $200 and up. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Lumbar pain is the most prevalent condition afflicting people today. Around 80 million people have problems with back pain at some stage in their life. It's a problem that costs businesses vast amounts of money year after year as a result of lost time and production. Innovative and better treatment solutions are continually sought after in the hope of lowering economical impact this issue causes.

People from all corners of the earth experience foot ache due to leg length discrepancy. In most of these cases Shoe Lifts can be of immense help. The lifts are capable of decreasing any discomfort in the feet. Shoe Lifts are recommended by numerous certified orthopaedic physicians.
To be able to support the body in a nicely balanced manner, your feet have got a vital role to play. In spite of that, it is often the most overlooked region of the body. Many people have flat-feet meaning there is unequal force exerted on the feet. This causes other parts of the body including knees, ankles and backs to be impacted too. Shoe Lifts make sure that proper posture and balance are restored.
Leg length inequality goes largely undiscovered on a daily basis, however this condition is simply corrected, and can reduce quite a few cases of low back pain.
Treatment for leg length inequality commonly consists of Shoe Lifts . Many are affordable, generally costing under twenty dollars, in comparison to a custom orthotic of $200 and up. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Lumbar pain is the most prevalent condition afflicting people today. Around 80 million people have problems with back pain at some stage in their life. It's a problem that costs businesses vast amounts of money year after year as a result of lost time and production. Innovative and better treatment solutions are continually sought after in the hope of lowering economical impact this issue causes.
People from all corners of the earth experience foot ache due to leg length discrepancy. In most of these cases Shoe Lifts can be of immense help. The lifts are capable of decreasing any discomfort in the feet. Shoe Lifts are recommended by numerous certified orthopaedic physicians.
To be able to support the body in a nicely balanced manner, your feet have got a vital role to play. In spite of that, it is often the most overlooked region of the body. Many people have flat-feet meaning there is unequal force exerted on the feet. This causes other parts of the body including knees, ankles and backs to be impacted too. Shoe Lifts make sure that proper posture and balance are restored.
What Is A Calcaneal Spur

Overview
Heel spurs, pointed, bony outgrowths of the heel, are caused by localized soft tissue inflammation and can be located at the back of the heel or under the heel, beneath the sole of the foot. Plantar fascitis is associated with inflammation caused by heel spurs on the soles of the feet. Both conditions are treated with ice application and anti-inflammatory medications. Orthotics may also provide some relief.
Causes
One frequent cause of injury to the plantar fascia is pronation. Pronation is defined as the inward and downward action of the foot that occurs while walking, so that the foot's arch flattens toward the ground (fallen arch). A condition known as excessive pronation creates a mechanical problem in the foot, and the portion of the plantar fascia attached to the heel bone can stretch and pull away from the bone. This damage can occur especially while walking and during athletic activities.

Symptoms
Pain and discomfort associated with heel spurs does not occur from the spur itself. The bone growth itself has no feeling. However, as you move, this growth digs into sensitive nerves and tissue along the heel of the foot, resulting in severe pain. Pain can also be generated when pushing off with the toes while walking. Swelling along the heel is also common.
Diagnosis
Most patients who are suffering with heel spurs can see them with an X-ray scan. They are normally hooked and extend into the heel. Some people who have heel spur may not even have noticeable symptoms, although could still be able to see a spur in an X-ray scan.
Non Surgical Treatment
Treatment of Heel Spurs is the same as treatment of plantar fasciitis. To arrive at an accurate diagnosis, our foot and ankle Chartered Physiotherapists will obtain your medical history and examine your foot. Throughout this process the physio will rule out all the possible causes for your heel pain other than plantar fasciitis. The following treatment may be used. Orthotics/Insoles. Inflammation reduction. Mobilisation. Taping and Strapping. Rest.
Surgical Treatment
Approximately 2% of people with painful heel spurs need surgery, meaning that 98 out of 100 people do well with the non-surgical treatments previously described. However, these treatments can sometimes be rather long and drawn out, and may become considerably expensive. Surgery should be considered when conservative treatment is unable to control and prevent the pain. If the pain goes away for a while, and continues to come back off and on, despite conservative treatments, surgery should be considered. If the pain really never goes away, but reaches a plateau, beyond which it does not improve despite conservative treatments, surgery should be considered. If the pain requires three or more injections of "cortisone" into the heel within a twelve month period, surgery should be considered.
Will A Calcaneal Spur Hurt?

Overview
A heel spur also known as a calcaneal spur, is a pointed bony outgrowth of the heel bone (calcaneus). Heel spurs do not always cause pain and often are discovered incidentally on X-rays taken for other problems. Heel spurs can occur at the back of the heel and also under the heel bone on the sole of the foot, where they may be associated with the painful foot condition plantar fasciitis.
Causes
A bone spur forms as the body tries to repair itself by building extra bone. It generally forms in response to pressure, rubbing, or stress that continues over a long period of time. Some bone spurs form as part of the aging process. As we age, the slippery tissue called cartilage that covers the ends of the bones within joints breaks down and eventually wears away (osteoarthritis). Bone spurs due to aging are especially common in the joints of the spine and feet.

Symptoms
Most heel spurs cause no symptoms and may go undetected for years. If they cause no pain or discomfort, they require no treatment. Occasionally, a bone spur will break off from the larger bone, becoming a ?loose body?, floating in a joint or embedding itself in the lining of the joint. This can cause pain and intermittent locking of the joint. In the case of heel spurs, sharp pain and discomfort is felt on the bottom of the foot or heel.
Diagnosis
Heel spurs and plantar fasciitis is usually diagnosed by your physiotherapist or sports doctor based on your symptoms, history and clinical examination. After confirming your heel spur or plantar fasciitis they will investigate WHY you are likely to be predisposed to heel spurs and develop a treatment plan to decrease your chance of future bouts. X-rays will show calcification or bone within the plantar fascia or at its insertion into the calcaneus. This is known as a calcaneal or heel spur. Ultrasound scans and MRI are used to identify any plantar fasciitis tears, inflammation or calcification. Pathology tests may identify spondyloarthritis, which can cause symptoms similar to plantar fasciitis.
Non Surgical Treatment
Exercise. If you think your pain is exercise-related, change your exercise routine, environment, or foot-ware, and emphasize movements and/or body parts that do not cause pain. Mind/Body. Occasionally foot pain can be related to stress. The body may respond with generalized tension that contributes to pain in many areas, including the feet. Hypnosis and guided imagery are worth exploring if an anatomical problem is not apparent. Supplements. Natural anti-inflammatories can be just as effective as ibuprofen or other over-the-counter pain relievers with fewer side effects. Try one of the following. Ginger (Zingiber officinale) standardized to 5-6% gingerols and 6% shogoals, take one to two 500 mg tablets three to four times daily. Turmeric (Curcuma longa) standardized to 95% curcuminoids, take 400-600 mg three times daily. Also, be sure that you're wearing well-fitting shoes, the proper shoes for each activity, and that you buy new foot-ware as soon as you notice signs of wear. You can also take the pressure off your heel with a donut-shaped heel cushion or a heel-raising pad placed in your shoe. Acupuncture can also relieve the pain, as can for some sufferers, magnetic shoe inserts, although the evidence behind their effectiveness is not conclusive. Osteopathic or chiropractic manipulation can help with soft tissue pain in and around the feet.
Surgical Treatment
Usually, heel spurs are curable with conservative treatment. If not, heel spurs are curable with surgery, although there is the possibility of them growing back. About 10% of those who continue to see a physician for plantar fascitis have it for more than a year. If there is limited success after approximately one year of conservative treatment, patients are often advised to have surgery.
Prevention
You can prevent heel spurs by wearing well-fitting shoes with shock-absorbent soles, rigid shanks, and supportive heel counters; choosing appropriate shoes for each physical activity; warming up and doing stretching exercises before each activity; and pacing yourself during the activities. Avoid wearing shoes with excessive wear on the heels and soles. If you are overweight, losing weight may also help prevent heel spurs.